
Professional Currency at 51: FREC Level 3 Revalidation, UKRC 2025 Amendments, and the Governance Risk of Competence Drift
Structured Recalibration, Evidence Alignment, and the Discipline of Operational Integrity in High-Responsibility Roles


Abstract
This article examines the decision to revalidate a FREC Level 3 qualification at 51 years of age in the context of the 2025 UK Resuscitation Council (UKRC) amendments. It argues that professional competence in high-responsibility roles is perishable and that failure to maintain alignment with evolving standards constitutes a governance risk. Using the CABCDE trauma framework and the ten-second catastrophic haemorrhage triage principle as analytical anchors, the article draws parallels between clinical prioritisation and organisational crisis leadership. It concludes that revalidation at senior level is not symbolic but a structural control measure reinforcing resilience integrity.

Introduction: Experience Without Recalibration
Professional longevity is frequently conflated with enduring competence. In high-consequence domains, emergency medicine, crisis leadership, infrastructure protection, this assumption is structurally unsound.
At 51, following a military career and more than two decades operating in complex environments across the Middle East, I chose to revalidate my FREC Level 3 qualification. The decision was not compliance-driven. It was prompted by the 2025 UKRC amendments and the recognition that standards evolution necessitates practitioner recalibration.
Competence that is not revalidated against current doctrine becomes historical competence. Historical competence may retain experiential value, but it does not guarantee alignment with contemporary evidence.
In governance terms, this represents competence drift.

Competence Drift as a Governance Failure
Drift in management systems is well documented: policy and practice gradually diverge unless actively reconciled. An analogous phenomenon occurs at practitioner level. Experience substitutes for evidence. Memory substitutes for updated protocol.
The UKRC 2025 amendments reflect accumulated international research and outcome data. Refinements to compression strategy, ventilation ratios, oxygen therapy thresholds, and early cardiac arrest decision-making alter intervention sequencing in measurable ways.
Where guidance changes, practitioner alignment must follow.
Failure to do so introduces risk at the point of execution, the moment when decision latency or mis-sequencing materially affects survival probability.
For organisations operating in remote industrial sites, energy infrastructure, or overseas deployments, first response capability may be internal for extended periods. In such contexts, outdated medical training is not a peripheral concern; it represents unmanaged liability exposure.
Revalidation is therefore not cosmetic. It functions as a preventive governance control.
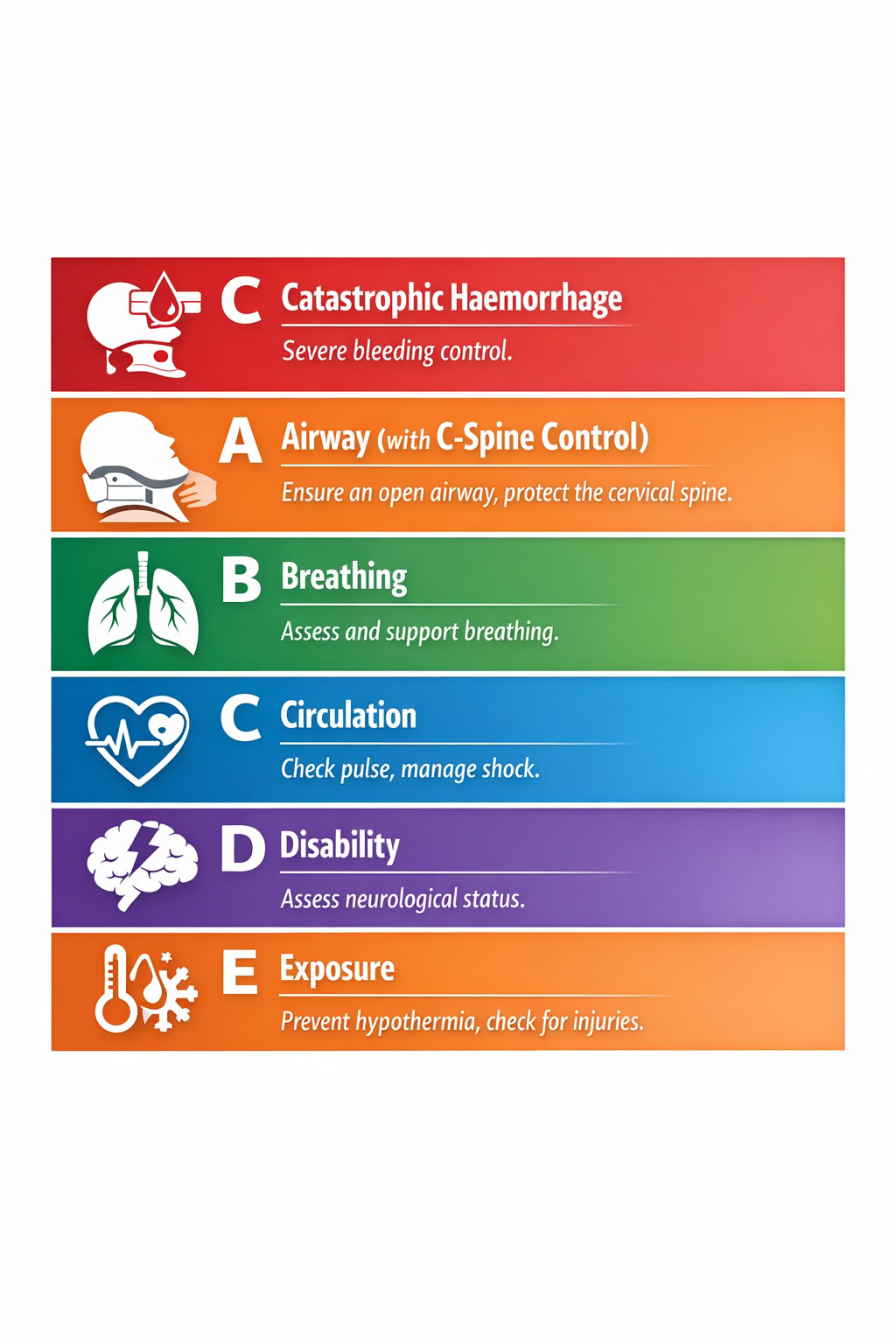
CABCDE: Structured Survival Logic
Central to FREC Level 3 trauma assessment is the CABCDE framework:
C – Catastrophic haemorrhage
A – Airway ( with C - Spine control)
B – Breathing
C – Circulation
D – Disability
E – Exposure
The explicit prioritisation of catastrophic haemorrhage reflects data drawn from trauma and conflict medicine: uncontrolled bleeding remains one of the most rapidly fatal yet preventable causes of death.
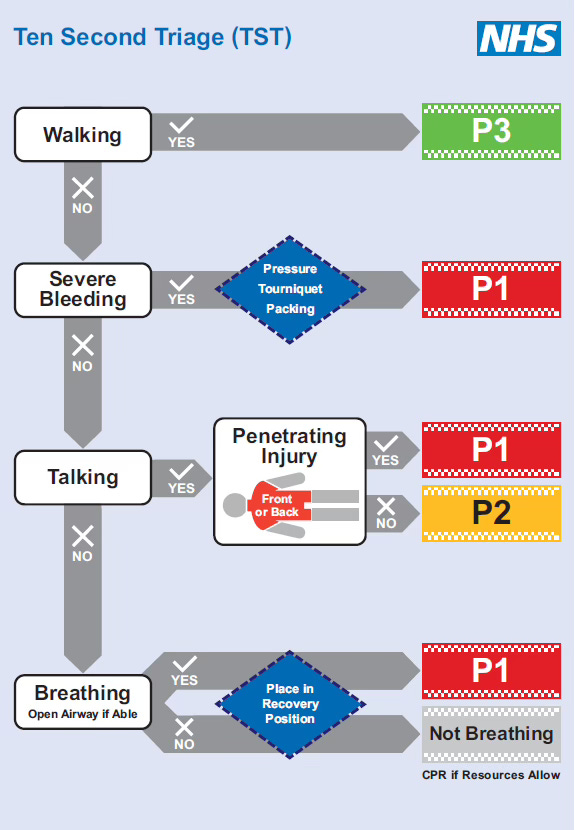
The framework is operationalised through the ten-second catastrophic haemorrhage sweep, a rapid triage discipline conducted before airway intervention.
The logic is non-negotiable:
Identify and control the condition that kills fastest before progressing to secondary assessment.
Tourniquet application, direct pressure, or haemostatic intervention precede airway adjuncts or oxygen delivery. The algorithm exists to remove cognitive delay under stress. It replaces instinct with structure.
The sequencing is evidence-driven prioritisation.
Translational Analysis: The Ten-Second Principle in Corporate Crisis
The CABCDE structure provides a direct analogue for organisational crisis governance.
During destabilising events, cyber breach, liquidity shock, regulatory enforcement, operational shutdown, leadership frequently mis-sequences response actions. Communication planning precedes exposure containment. Stakeholder management precedes technical stabilisation.
The clinical principle demands a different discipline:
What kills the system first?
In corporate terms, the catastrophic risk (“C”) may manifest as:
Insolvency exposure
Data exfiltration
Licence suspension
Infrastructure failure
Failure to identify and stabilise that primary threat renders downstream interventions secondary and, in extreme cases, irrelevant.
The ten-second triage mindset therefore functions as a decision-making model: identify the existential risk immediately and stabilise it before progressing.
At Pillars Global, resilience architecture is built upon this prioritisation logic, structured escalation pathways that stabilise catastrophic exposure before expanding response layers.

Senior Revalidation as Cultural Control
ISO-aligned management systems consistently emphasise competence maintenance and continual improvement. Yet cultural erosion often begins when senior practitioners assume experiential exemption from revalidation.
This exemption weakens system integrity.
Revalidation at senior level communicates structural consistency:
Standards evolve and must be tracked.
Evidence supersedes tenure.
Competence is demonstrable, not presumed.
The act of requalification therefore operates as cultural governance, reinforcing alignment between documented expectation and behavioural practice.

Static Certification Versus Dynamic Capability
Certification confirms prior assessment at a defined time. Capability confirms present readiness under current standards.
Emergency medical practice illustrates this distinction starkly. Outdated compression depth or ventilation sequencing measurably affects outcome probability. The tolerance for legacy knowledge is minimal.
Organisational crisis governance is subject to the same constraint. Threat vectors evolve. Regulatory frameworks shift. Geopolitical risk recalibrates. Static response models degrade in relevance.
Competence decay is gradual and largely invisible until tested.
Revalidation interrupts that decay cycle.

Implications for Resilience Practice
The 2025 UKRC amendments serve as a practical reminder that resilience disciplines, clinical or corporate, are evidence-responsive systems. Professional credibility requires active alignment with that evidence.
Within Pillars Global, resilience is treated as an engineered construct comprising structured prioritisation, dynamic reassessment, and disciplined execution. Revalidating FREC Level 3 aligns personal capability with the same principles embedded in advisory frameworks.
If resilience systems are to maintain integrity, practitioners must model the same review discipline they recommend.

Conclusion
Professional competence in high-responsibility domains is perishable. Absent structured recalibration, divergence from evolving standards is inevitable.
Revalidating FREC Level 3 at 51, in alignment with the 2025 UKRC amendments, was not an act of renewal for its own sake. It was a governance decision: a control measure against competence drift and a reinforcement of prioritised response logic.
CABCDE and the ten-second catastrophic haemorrhage principle represent disciplined sequencing under pressure. The same logic underpins effective crisis leadership.
In both clinical response and organisational governance, integrity is measured not by past exposure but by present alignment with current evidence.
Professional longevity does not remove that obligation.
It intensifies it.